Annual Report 2024
Department of Esophageal Surgery
Takeo Fujita M.D./Ph.D., Naoto Fujiwara M.D./Ph.D., Kazuma Sato M.D./Ph.D.
Introduction
The Department of Esophageal Surgery deals with neoplasms arising from the esophagus. The surgical management of esophageal cancer has been the primary clinical and research activity of this department. In particular, our department is striving to establish minimally invasive surgery that consists of neoadjuvant treatment followed by minimally invasive esophagectomy. Our department is conducting a study to define the role of surgery in the multimodal approach to the treatment of esophageal cancer, and is aiming for thoraco-laparoscopic esophagectomy, which consists of thoracoscopic esophagectomy and laparoscopic reconstruction, to become a standard surgical procedure.
The Team and What We Do
In our department, we performed about 160 cases of thoracoscopic surgery for esophageal cancer in 2024, with a particular focus on robotic surgery. In addition, robotic surgery has become the standard procedure for abdominal operations, replacing laparoscopic surgery. Alongside these, in recent years we have been actively introducing mediastinoscopy for very elderly patients over the age of 85 and for cases with poor tolerance of thoracotomy.
In addition, we perform multidisciplinary treatment, including preoperative treatment, for cervical esophageal cancer in collaboration with plastic surgery, and in 2024, we performed radical surgery for 9 cases of cervical esophageal cancer, and of these, we performed larynx-sparing cervical esophageal surgery for 6 cases, including cases in which a response was obtained through preoperative chemotherapy, etc. In the future, it is expected that Japan as a whole will move beyond being a super-aged society and enter a period of being a society with a very high proportion of elderly people. As the number of esophageal cancer surgery cases increases with the aging of the population, it is important to provide individualized minimally invasive surgery for the elderly, depending on their physical functions and the degree of tumor progression, therefore we are working to provide safe surgical treatment that maintains quality of life. In recent years, we have also actively introduced robot-assisted esophageal surgery to further reduce invasiveness, and in 2024 we performed over 120 cases under robot-assisted surgery. In 2022, we also introduced robot-assisted trans-cervical mediastinoscopic esophagectomy (RACE), which is still rarely used worldwide, and by March 2025 we had performed 50 cases, with good results.
In addition to JCOG activities, we are also conducting research on gastric blood flow evaluation using oxygen saturation imaging technology to evaluate the optimal anastomotic site, and research on evaluating blood flow in reconstructed organs using tissue oxygen saturation and hemoglobin index. We are also conducting research on intraoperative AI analysis of the recurrent nerve using deep learning methods, which have been developed significantly in recent years.
Table 1. Type of Procedures for Thoracic Esophageal Cancer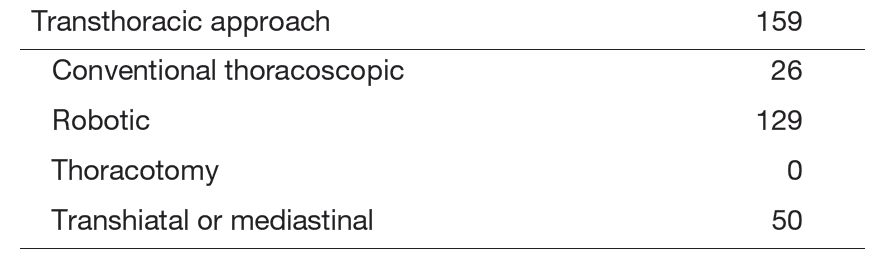
Table 2. Type of Procedures for Cervical Esophageal Cancer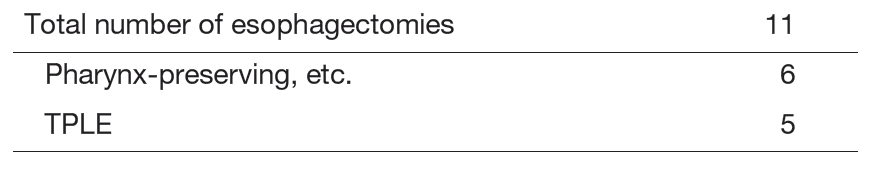
Research Activities
To achieve the best practice for patients, we are investigating several aspects of tissue perfusion imaging study. First, we use the O2 saturation imaging to explore the best gastric conduit and the most suitable anastomotic site during surgery. Second, we use AI deep learning technology to focus on AI-guided real time surgery particularly for the anatomical recognition of recurrent laryngeal nerves to avoid unexpected injury and subsequent recurrent nerve palsy which greatly impair the patients’ quality of life after surgery. Third, conferring with the preoperative patients and their families, we are conducting a case control, investigating whether or not an active preoperative rehabilitation program with a nutrition program would improve the postoperative patients’ status, particularly skeletal mass index (which is vital to avoid sarcopenia), and reduce the postoperative fatigue. Several other research activities are planned at this point. We are also currently submitting a paper on intraoperative AI analysis of the recurrent nerve.
Clinical Trials
Currently, our department is examining the role of thoracolaparoscopic esophagectomy as a minimally invasive esophagectomy that consists of thoracoscopic esophagectomy and laparoscopic reconstruction. For patients without radical chemoradiotherapy, thoracoscopic esophagectomy in the prone position with radical lymph node dissection and laparoscopic reconstruction after esophagectomy for patients without a history of laparotomy are performed to determine their role as standard surgical procedures for esophageal cancer. For treating patients aged over 80 years or at high risk, a two-stage surgical procedure divided into resection and reconstruction is being conducted.
A randomized controlled phase III study comparing cisplatin and 5-fluorouracil versus
cisplatin and 5-fluorouracil plus docetaxel versus cisplatin and 5-fluorouracil with concurrent radiation as a neoadjuvant treatment for locally advanced esophageal cancer is ongoing. A randomized controlled phase III study of minimally invasive versus open esophagectomy for thoracic esophageal cancer (JCOG1409, MONET trial) is ongoing.
Furthermore, a randomized controlled phase III study comparing induction treatment with cisplatin and 5-fluorouracil plus docetaxel and subsequent conversion surgery versus cisplatin and 5-fluorouracil with concurrent radiation as a definitive treatment for locally advanced (cT4b or borderline tumor) esophageal cancer is ongoing. A randomized controlled phase III study of minimally invasive versus open esophagectomy for thoracic esophageal cancer (JCOG1510, TRIANgLE trial) is ongoing. Since 2000, our department has started performing salvage surgery for patients with unsuccessful definitive chemoradiotherapy. The operative procedures and postoperative management have been refined gradually. Our department is also studying the role and efficacy of salvage surgery in the multimodal treatment of esophageal cancer.
Education
In academic training, we teach our residents not only about surgical practice but also several aspects of academic activities for PhD course students. As the National Cancer Center attracts excellent young physicians from all over the country, it is important that they make full use of the center's resident program to gain a thorough understanding of the role of esophageal surgery in cancer treatment and diagnosis. In addition to the usual surgical training, we also provide education through patient education classes with a range of different professionals. In terms of research, in 2024, one resident specializing in cancer treatment obtained a degree from the Cancer Center and the affiliated graduate school, and a graduate student from the affiliated graduate school is conducting research for a degree. One graduate of our department has obtained a specialist qualification in esophageal surgery. In addition, one resident specializing in cancer treatment and one resident have obtained specialist qualifications in surgical treatment for gastrointestinal cancer and certification in surgical treatment for gastrointestinal cancer.
Future Prospects
We are exploring the best clinical practice for patients and their families. To achieve this mission, we will continue to explore the best surgical practice and future research activities conducted in cooperation with other domestic and international research institutes.
List of papers published in 2024
Journal
1. Matsuda S, Takeuchi H, Kato K, Machida R, Ito Y, Tsubosa Y, Daiko H, Koyanagi K, Ogata T, Fukuda T, Fujita T, Abe T, Bamba T, Watanabe M, Kawakubo H, Shibuya Y, Otsubo D, Kakisita T, Hashimoto T, Sasaki K, Kitagawa Y. Prognostic Impact of Thoracic Duct Resection in Patients Who Underwent Transthoracic Esophagectomy Following Neoadjuvant Therapy for Esophageal Squamous Cell Carcinoma: Exploratory Analysis of JCOG1109. Annals of surgical oncology, 32:293-301, 2025
2. Oda S, Kuno H, Fujita T, Hiyama T, Kotani D, Kadota T, Sakashita S, Kobayashi T. Clinical usefulness of four-dimensional dynamic ventilation CT for borderline resectable locally advanced esophageal cancer. Japanese journal of radiology, 43:434-444, 2025
3. Kooij CD, de Jongh C, Kingma BF, van Berge Henegouwen MI, Gisbertz SS, Chao YK, Chiu PW, Rouanet P, Mourregot A, Immanuel A, Mala T, van Boxel GI, Carter NC, Li H, Fuchs HF, Bruns CJ, Giacopuzzi S, Kalff JC, Hölzen JP, Juratli MA, Benedix F, Lorenz E, Egberts JH, Haveman JW, van Etten B, Müller BP, Grimminger PP, Berlth F, Piessen G, van den Berg JW, Milone M, Luketich JD, Sarkaria IS, Sallum RAA, van Det MJ, Kouwenhoven EA, Brüwer M, Harustiak T, Kinoshita T, Fujita T, Daiko H, Li Z, Ruurda JP, van Hillegersberg R. The Current State of Robot-Assisted Minimally Invasive Esophagectomy (RAMIE): Outcomes from the Upper GI International Robotic Association (UGIRA) Esophageal Registry. Annals of surgical oncology, 32:823-833, 2025
4. Tomi Y, Kinoshita T, Yura M, Sakamoto N, Fujita T, Tokunaga M, Kinugasa Y. Accuracy of the preoperative estimation of esophageal invasion length of adenocarcinoma of the esophagogastric junction and its discrepancy with the pathological measurement. Surgery today, 55:768-777, 2025
5. Harada T, Tsuji T, Ueno J, Konishi N, Yanagisawa T, HIjikata N, Ishikawa A, Hashimoto K, Kagaya H, Tatematsu N, Zenda S, Kotani D, Kojima T, Fujita T. Clinical mechanism of muscle mass loss during neoadjuvant chemotherapy in older patients with esophageal cancer: a prospective cohort study. Diseases of the esophagus, 38:doae096, 2025
6. Kajiyama D, Fujiwara N, Shigeno T, Sato K, Yamaguchi M, Sakashita S, Daiko H, Fujita T. Impact of Lymphatic and Venous Invasion Patterns on Postoperative Prognosis and Distant Metastasis in Esophageal Squamous Cell Carcinoma After Preoperative Chemotherapy. Annals of surgical oncology, 32:860-871, 2025
7. Kajiyama D, Fujiwara N, Yamaguchi M, Daiko H, Fujita T. ASO Author Reflections: Impact of Lymphatic and Venous Invasion Patterns on Postoperative Prognosis in Esophageal Squamous Cell Carcinoma. Annals of surgical oncology, 32:882-883, 2025
8. Harada T, Tsuji T, Fukushima T, Konishi N, Nakajima H, Suzuki K, Ikeda T, Toyama S, Matsumori K, Yanagisawa T, Hashimoto K, Kagaya H, Zenda S, Kojima T, Fujita T, Ueno J, Hijikata N, Ishikawa A, Hayashi R. Current status of prehabilitation before esophagectomy for patients with esophageal cancer among board-certified hospitals by the Japan Esophageal Society. Esophagus, 22:340-348, 2025
9. Takei S, Kotani D, Laliotis G, Sato K, Fujiwara N, Kawazoe A, Hashimoto T, Mishima S, Nakayama I, Nakamura Y, Bando H, Kuboki Y, Sakashita S, Spickard E, George GV, Dutta P, Sharma S, Malhotra M, Sethi H, Jurdi A, Liu MC, Yoshino T, Shitara K, Kojima T, Fujita T. Circulating Tumor DNA Assessment to Predict Risk of Recurrence after Surgery in Patients with Locally Advanced Esophageal Squamous Cell Carcinoma: A Prospective Observational Study. Annals of surgery, 2025
10. Fujita T, Sato K, Kajiyama D, Kubo Y, Fujiwara N, Daiko H. Short-and middle-term outcomes of robot-assisted minimally invasive esophagectomy for highly locally advanced esophageal cancer with stage cT3 borderline and cT4b at initial diagnosis. Surgical endoscopy, 39:2994-3005, 2025
11. Kajiyama D, Fujiwara N, Shigeno T, Sato K, Yamaguchi M, Sakashita S, Daiko H, Fujita T. ASO Visual Abstract: Impact of Lymphatic and Venous Invasion Patterns on Postoperative Prognosis and Distant Metastasis in Esophageal Squamous Cell Carcinoma After Preoperative Chemotherapy. Annals of surgical oncology, 32:894-895, 2025
12. Harada T, Tsuji T, Yanagisawa T, Ueno J, Hijikata N, Ishikawa A, Hiroshige K, Kotani D, Kojima T, Fujita T. Skeletal muscle mass recovery after oesophagectomy and neoadjuvant chemotherapy in oesophageal cancer: retrospective cohort study. BMJ supportive & palliative care, 14:326-334, 2024
13. Daiko H, Oguma J, Ishiyama K, Kurita D, Kubo K, Kubo Y, Utsunomiya D, Igaue S, Nozaki R, Leng XF, Fujita T, Fujiwara H. Technical feasibility and oncological outcomes of robotic esophagectomy compared with conventional thoracoscopic esophagectomy for clinical T3 or T4 locally advanced esophageal cancer: a propensity-matched analysis. Surgical endoscopy, 38:3590-3601, 2024
14. Kubo Y, Kajiyama D, Sato K, Fujita T. Therapeutic Strategy by Neuronal Pentraxin Receptor for Esophageal Squamous Cancer Cells. Annals of surgical oncology, 31:5493-5494, 2024
15. Shigeno T, Kajiyama D, Sato K, Fujiwara N, Kinugasa Y, Daiko H, Fujita T. Efficiency of conversion surgery for esophageal squamous cell carcinoma with solitary abdominal para-aortic lymph node metastasis. Surgery today, 54:1490-1497, 2024
16. Sato K, Fujita T, Otomo M, Shigeno T, Kajiyama D, Fujiwara N, Daiko H. Total RAMIE with three-field lymph node dissection by a simultaneous two-team approach using a new docking method for esophageal cancer. Surgical endoscopy, 38:4887-4893, 2024
17. Harada T, Tsuji T, Fukushima T, Ikeda T, Toyama S, Konishi N, Nakajima H, Suzuki K, Matsumori K, Yanagisawa T, Hashimoto K, Kagaya H, Zenda S, Kojima T, Fujita T, Ueno J, Hijikata N, Ishikawa A, Hayashi R. The implementation status of prehabilitation during neoadjuvant chemotherapy for patients with locally advanced esophageal cancer: a questionnaire survey to the board-certified facilities in Japan. Esophagus, 21:496-504, 2024
18. Shigeno T, Otomo M, Kajiyama D, Sato K, Fujiwara N, Kinugasa Y, Daiko H, Fujita T. Assessing the outcomes of posterior thoracic para-aortic lymph node dissection after induction chemotherapy in patients with esophageal squamous cell carcinoma. Diseases of the esophagus, 37:doae060, 2024
19. Daiko H, Ishiyama K, Kurita D, Kubo K, Kubo Y, Utsunomiya D, Igaue S, Nozaki R, Akimoto E, Kakuta R, Horonushi S, Fujita T, Oguma J. Bilateral transcervical mediastinoscopic-assisted transhiatal laparoscopic esophagectomy compared with thoracolaparoscopic esophagectomy for esophageal cancer: a propensity score-matched analysis. Surgical endoscopy, 38:5746-5755, 2024
20. Tanaka K, Fujita T, Nakajima Y, Okamura A, Kawada K, Watanabe M, Doki Y. Validation of the cutoff values for the number of metastatic lymph nodes for esophageal cancer staging: a multi-institutional analysis of 655 patients in Japan. Esophagus, 21:464-471, 2024
21. Fujita T, Sato K, Fujiwara N, Kajiyama D, Kubo Y, Daiko H. Robot-assisted cervical esophagectomy with simultaneous transhiatal abdominal procedure for thoracic esophageal carcinoma. Surgical endoscopy, 38:6413-6422, 2024
22. Minakata N, Kadota T, Sakashita S, Inaba A, Sunakawa H, Takashima K, Nakajo K, Murano T, Shinmura K, Yoda Y, Ikematsu H, Fujita T, Kinoshita T, Yano T. Tumor thickness is associated with metastasis in patients with submucosal invasive adenocarcinoma of the esophagogastric junction. Diseases of the esophagus, 37:doae083, 2024
23. Fujita T, Sato K, Fujiwara N, Shigeno T. Imaging technology to assess tissue oxygen saturation of the gastric conduit in thoracic esophagectomy. JTCVS techniques, 28:173-176, 2024
24. Harada T, Tsuji T, Ueno J, Konishi N, Yanagisawa T, Hijikata N, Ishikawa A, Hashimoto K, Kagaya H, Tatematsu N, Zenda S, Kotani D, Kojima T, Fujita T. Association of Preoperative Physical Fitness With Post-Esophagectomy Pneumonia in Older With Locally Advanced Esophageal Cancer: An Exploratory Prospective Study. Journal of surgical oncology, 2024